Catholic Medical Quartery Vol 76 (1) February 2026
Promoting risky unprotected sex is not a breakthrough for women's rights!
Lucy Marsh. Communications and PR Officer, Family Education Trust
 Pharmacists
shouldn't be handing out the morning after pill!
Pharmacists
shouldn't be handing out the morning after pill!
Free morning after
pills from pharmacies are a bad idea
The Health Secretary Wes Streeting recently announced on X (Twitter) that emergency contraceptives will now be available to women at pharmacies. He said, “This is biggest change to sexual health services since the 1960s and a major advance for women’s reproductive health” and went on to complain about negative replies to his post, tweeting in a follow up post, “A reminder that, at a time when women’s reproductive health and rights are under attack, Labour will always defend them.”
The NHS information page says that the oral emergency contraception pill will be available for free to women from almost 10,000 pharmacies across the country without needing to see their GP or get an appointment at a sexual health clinic.
Those of us who think this is a bad idea are not “attacking women” — we believe that this policy development promotes risky sexual behaviour and separates sex from its procreative function. This is not in the best interests of women and girls, since women are more likely to suffer physical consequences and emotional distress from engaging in casual sex.
Risky sexual behaviour impacts on mental health
One in three 17 to 19-year-old young women are suffering with mental health issues, more than twice the proportion of young men the same age. Today’s young people have the poorest mental health of any age group in the UK, whereas two decades ago the reverse was true. A third of young adults aged 18–24 are reporting symptoms of “common mental disorders” (e.g. anxiety and/or depression). This figure rises to 41% for young women.
A 2023 study of young adults in Sweden found that young women aged 18-30 with depression were more likely to have multiple sexual partners. The researchers concluded that further research is needed to understand how risky sexual behaviour, especially multiple sexual partners, impacts on mental health in order “to support evidence-based interventions.”
Another 2023 article states that various studies have shown that those with multiple sexual partners have a higher chance of experiencing mental health disorders, as well as having sexual intercourse in early adolescence being linked to mental health outcomes.
Meanwhile, rather than discouraging promiscuity, the UK Government’s plan is to increase easy access to emergency contraception, despite the significant increase in sexually transmitted infections (STIs) in recent years.
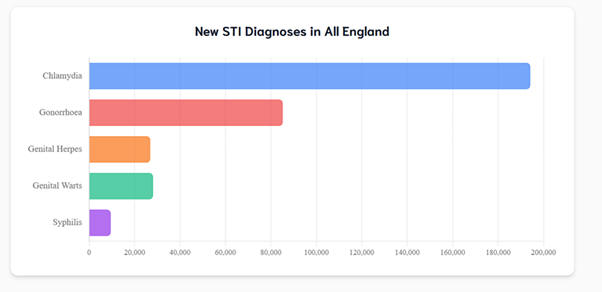
STIs are a huge problem
The most recent data from the UK Health Security Agency (UKHSA) published in June showed that syphilis cases in England are now at the highest number reported since 1948, with diagnoses increasing by 5% from 12,456 in 2023 to 13,030 in 2024.
While gonorrhoea cases decreased by almost 16% last year, the UKHSA said “it is too soon to conclude whether this trend will continue” and warned there is a worrying “acceleration in diagnoses of antibiotic-resistant gonorrhoea cases” this year.
Rates of sexually transmitted infections (STIs) are highest in young people aged 15 to 24 years, with more than 350 diagnoses every day in this age group in 2024. The UKHSA issued advice to students in September, warning them to use condoms and to get tested if having unprotected sex with new partners.
Sexual health charity Brook was quoted in UKHSA’s press release, with Laura Domegan, Brook’s Head of Nursing saying, “we want students starting a new university to be feel confident discussing condoms with the people they are having sex with.”
The key factor is the phrase “people” they are having sex with, rather than “person” or “partner.” Casual sex has become so normalised that it’s assumed students will be sleeping around with multiple people. The alarming rise in STIs in this age group would suggest that this is indeed the case.
Casual sex with multiple partners has been normalised
Brook, and indeed the Government, do not appear to regard this as a problem. On its advice pages about casual sex, Brook states: “Casual relationships have become popular and can be great” and “can offer intimacy, pleasure, friendship, emotional support and fun”.
If you type the word “monogamy” into Brook’s search bar it comes up with a page on Polyamory and non-monogamous relationships. Its “Our Beliefs” section states mandatory relationship and sex education (RHSE) should address “all sexual activity throughout the life course as worthy of care, mutual respect and most importantly enthusiastic consent” and urges that there must be “an end to the idea of virginity as an important state or something that tells us anything about a person’s worth or personal values.”
Bearing in mind that Brook and the Family Planning Association, contributed to the consultation process which made RHSE mandatory in all schools in 2019, it’s unsurprising that there’s a disproportionate prevalence of STIs among young people, when they are told the only thing that matters about sex is consent and pleasure.
Brook informs 13-15 year olds, that while sex under 16 is unlawful, “it’s highly unlikely you will get into trouble with the law as long as there is not a large age difference between you and your partner and you both agree (consent) to sex.” It adds that “the most important thing to remember is that sex should be something you want and feel comfortable with” — and signposts under 16s to confidential sexual health services.
Patient group directions are Trust policies that enable the provision of morning after pill (Emergency Hormonal Contraception) for females as young as 13 by professionals such as pharmacists. A sample Patient Group Direction is seen below.
Figure 1 is an example of the National Patient Group Direction for emergency contraception
| Management of the National Patient Group Direction (PGD) |
The original signed copy should be held by the NHS Board. This PGD must be read, agreed to and signed and a copy retained by all staff involved in its use. The original signed copy should be held by the Health Board. |
| Application |
This PGD covers the supply of, levonorgestrel 1500mcg tablet (Levonelle R 1500) for use as emergency hormonal contraception by female patients who are aged 13 years or over, provided none of the exclusion criteria listed below apply. |
| Situation |
Patient presenting in person at the community Pharmacy requesting emergency contraception for their own use within 72 hours of unprotected sexual intercourse (UPSI), |
| Inclusion Criteria |
Patient is aged 13 years or over. Unprotected sexual intercourse/contraception failure within the last 72 hours. Unprotected sexual intercourse/contraception failure within the last 72 hours where patient has vomited within 2 hours of taking a dose of Levonorgestral for emergency hormonal contraception. Patient gives their consent to providing the relevant clinical information to the pharmacist after the pharmacist has assessed their capacity to consent (see under staff). |
| Exclsion Criteria |
Patient is aged 12 years or under. The Child Protection Team must be contacted for children of 12 years and under, who present having had sexual intercourse. Patient who the pharmacist has assessed as not being competent to consent. Unexplained vaginal bleeding. Patient has had unprotected sex more than 72 hours ago. Levonogestrel should not be given to pregnant women. Previous unprotected sexual intercourse in current menstrual cycle. Patient used levonorgestrel for emergency hormonal contraception in current menstrual cycle. (If patient has vomited within 2 hours of taking a dose of levonorgestrel, dose can be repeated. Refer to Inclusion Criteria. Severe hepatic dysfunction. Severe malabsorption syndromes e.g. severe diarrhoea, Crohns disease. Porphyria Hypersensitivity to levonorgestrel or any of the tablet ingredients/ excipients (potato starch, maize starch, colloidal silica anhydrous, magnesium stearate, talc, lactose monohydrate). Patients who have delivered a baby within last 3 weeks (EHC not required in these circumstances). Patient does not agree to share relevant clinical information or there is no valid consent. Patients with hereditary problems of galactose intolerance |
In 2014, our former Trustee Sarah Carter warned the Education Select Committee that Brook’s “traffic light safeguarding tool” described 13-17 year old children having “consenting oral and/or penetrative sex with others of similar age and developmental ability” as a “safe and healthy sexual development.” IDAS, which offers free and confidential services to help people cope with domestic abuse and sexual violence, says that “young people are unlikely to be prosecuted for mutually agreed sexual activity where there is no evidence of exploitation” and adds that children “have a right to confidential advice on contraception, pregnancy and abortion.”
Gillick competence has gone too far
Underage sex is now become so normalised that NHS guidelines state that emergency contraception can be prescribed to girls aged 13 provided they are judged by professionals to be Gillick competent. This means that if a doctor or nurse finds that a child under 16 has understood the information, risks and benefits, they can receive medical treatment without permission from their parents or carers, even if their parents or carers do not want them to have the treatment.
The Teen Health website states that “The Sexual Offences Act 2003 recognises that young people under 16 may have consensual sex with partners of a similar age. The law does not seek to prosecute where this is the case unless there is a risk of harm.” It adds that “young people under 13, can't consent to sex and this would be considered a very serious offence”, thus implying there is no intrinsic harm in children under 16 being sexually active unless they are being coerced.
Despite the legal age of consent being 16, current NHS guidelines say that girls as young as 13 can be prescribed hormonal contraception without the knowledge or consent of their parents. 13-year-old girls can also seek advice for pregnancy and be referred for an abortion without any health professional telling their parents.
GMC guidelines instruct doctors that they “can provide contraceptive, abortion and STI advice and treatment, without parental knowledge or consent, to young people under 16 provided that:
They understand all aspects of the advice and its implications.
You cannot persuade the young person to tell their parents or to allow you to tell them
In relation to contraception and STIs, the young person is very likely to have sex with or without such treatment
Their physical or mental health is likely to suffer unless they receive such advice or treat ment, and;
It is in the best interests of the young person to receive the advice and treatment without parental knowledge or consent.”
The Gillick ruling is pernicious
and something that we will examine in our soonto-be-published updated version of our 2017 report Unprotected, which looked at how underage sex has become normalised.
In the report, our late Director Norman examined the serious case reviews into several towns and looked at the reasons why the adults meant to protect them accepted that vulnerable girls aged as young as 11 could ‘consent’ to sex. Instead of automatically realising that children this age were being sexually abused, police dismissed the girls as promiscuous, local authorities turned a blind eye and medical professionals handed out contraceptives and referred girls for abortions.
In January 2025, a group of MPs wrote to Wes Streeting explaining that sexual abusers can more easily hide their crimes because there is no automatic requirement for clinics to notify a parent or guardian before performing an abortion on a child.
Father of the House and former minister, Sir Edward Leigh MP said it was clear that the “current abortion laws made it far easier to conceal these crimes. They should be revisited urgently to prevent further catastrophes on this scale.”
Instead of addressing how current laws on underage sex and abortion enable child grooming and sexual exploitation to be concealed, the Government has now made it even easier for sexual predators to cover up their crimes by simply visit- ing a pharmacy to obtain the morning after pill.
What can be done?
We need to rethink how society views sexual behaviour, children, parental responsibility and the law. If we continue treating young people as fully autonomous with sexual rights and overlook parental involvement, underage sex will continue to be normalised and children may face greater risks.
As Norman concluded in Unprotected, “If we treat the family unit as an irrelevance in the services we offer to children and young people, we are removing them from a vital accountability structure. We are also encouraging them to think and act in an individualistic way that will not help them to see the value of a supportive family network when they have children of their own.”
Lucy
Marsh is Communications and
PR Office of the Family Education Trust