Was a tension haemothorax the cause of Christ’s effusion of blood?
Professor Patrick Pullicino
Abstract
The hypothesis is advanced that the effusion of blood and water from Christ’s side were a consequence of his shoulder wound and that a tension Was a tension haemothorax the cause of Christ’s effusion of blood?haemothorax was the cause of the blood effusion. From measurements of the right upper limb on the Turin shroud, Bevilacqua et al. recently concluded that the “shroud man” suffered an extensive brachial plexus avulsion in association with an infra-glenoid shoulder dislocation. The dislocation and denervation of the right shoulder and arm muscles predisposed the right subclavian/ axillary artery to stretch injury. Since the subclavian artery exits the thorax over the first rib, it is postulated that the repeated raising and lowering of the body to breathe, caused repeated friction of the stretched subclavian artery over the first rib. This led to the artery’s eventual rupture and tension haemothorax, which was the source of the effusion of blood. It is further hypothesized that the effusion of water might have originated from a localised extra-pleural cerebrospinal fluid collection. Tracking of cerebrospinal fluid to the paraspinal and peri-pleural space adjacent to the upper lung is a documented complication of brachial plexus avulsion.
The Evidence
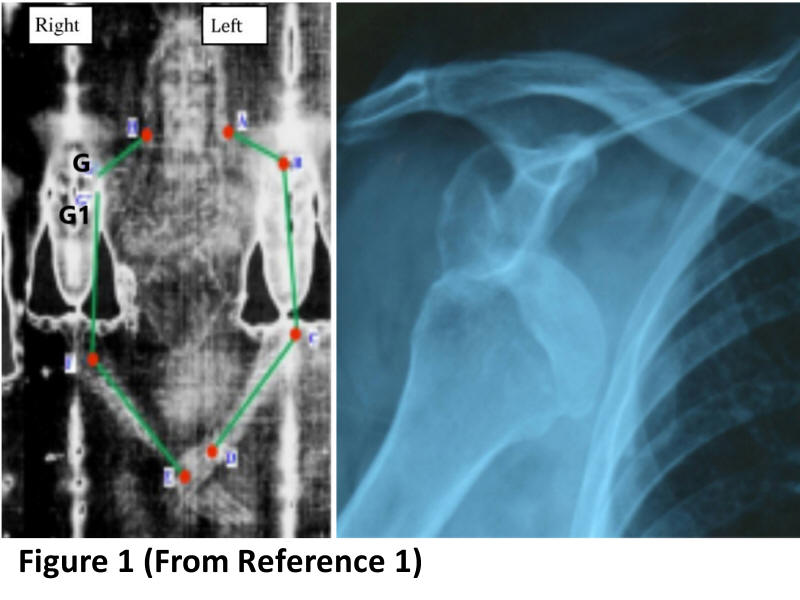
After making careful measurements on the Turin shroud, Bevilacqua et al [1] recently concluded that the “shroud man” suffered an extensive right brachial plexus avulsion injury. This is based on two observations: Firstly, that the right humerus is 3.5 cm below the shoulder (G1-G in Figure 1). They conclude this is due to an infra-glenoid dislocation. The cause of this dislocation was likely due to a fall when the cross was being carried on the right side. As a result of the fall, the “shroud man’s” shoulder became trapped between a supporting strut and the patibulum (they say that Christ used a T-shaped cross which had struts supporting the arms of the patibulum on each side [2]). The cross then fell across his back causing a violent upward pulling of his arm and the dislocation. Secondly their measurements also show that the whole right shoulder is depressed (G-H compared to A-B in figure 1) also the right hand is flat with straightened fingers. These findings, they attribute to loss of power of the neck, shoulder and hand muscles secondary to an extensive (upper and lower) brachial plexus avulsion. They hypothesise that the patibulum of the cross struck the back of the “shroud man” between the neck and shoulder and caused a displacement of his head to the left. This resulted in avulsion of both upper and lower parts of the right brachial plexus.
 As
seen in Figure 1, as a result of these injuries the right arm is displaced
downwards and the finger-tips of the right hand reach the left lateral
thigh. Measurements taken on Bevilaqua’s figure 1 reveal that the right
wrist (point E) is about 5cm vertically lower than the left wrist (point
D). In addition, the right finger-tips project about 10cm closer to the
lateral thigh than the left finger-tips (Figure 1 ). This shows that the
right arm was stretched to greater than its normal length during
crucifixion which was facilitated by a combination of shoulder dislocation
and loss of shoulder muscle power.
As
seen in Figure 1, as a result of these injuries the right arm is displaced
downwards and the finger-tips of the right hand reach the left lateral
thigh. Measurements taken on Bevilaqua’s figure 1 reveal that the right
wrist (point E) is about 5cm vertically lower than the left wrist (point
D). In addition, the right finger-tips project about 10cm closer to the
lateral thigh than the left finger-tips (Figure 1 ). This shows that the
right arm was stretched to greater than its normal length during
crucifixion which was facilitated by a combination of shoulder dislocation
and loss of shoulder muscle power.
The current paper proposes that because of this right arm stretching,
the right subclavian/ axillary artery was also subjected to stretch, as it
was one of the only remaining intact structures connecting the body and
the right arm. Anatomically, the right subclavian artery leaves the thorax
passing over the first rib, contacting its upper surface in the subclavian
groove. It then forms the axillary and then brachial artery. Inhalation
and exhalation during crucifixion necessitates extension and flexion of
elbows, abduction and adduction of shoulders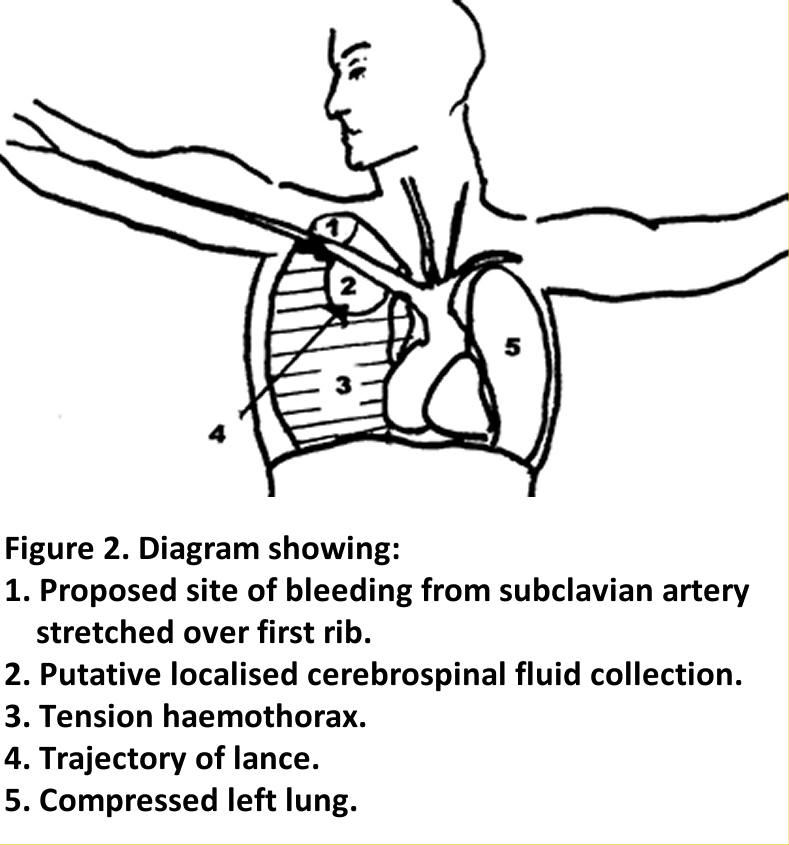 and alternate transferring of weight between the arms and legs. [3]
Transferring of body weight to the arms in inspiration, is likely to have
caused further stretching of the right subclavian artery. Transferring
weight to the legs in exhalation, would reverse this stretch. This would
cause the stretched subclavian artery to move across the first rib surface
with each breath, and its underside would be subject to friction. This
paper postulates that over the course of three hours, the subclavian
artery became abraded, injured and its wall attenuated, until finally the
artery ruptured and profuse bleeding ensued. It is likely that bleeding
was directed downwards and caused a large tension haemothorax (figure 2),
as occurred in rupture of a subclavian aneurysm reported in the
literature.[4] Tension haemothorax can contain up to 40% of the
circulating blood volume [5] and may lead to fatal circulatory
collapse[6].
and alternate transferring of weight between the arms and legs. [3]
Transferring of body weight to the arms in inspiration, is likely to have
caused further stretching of the right subclavian artery. Transferring
weight to the legs in exhalation, would reverse this stretch. This would
cause the stretched subclavian artery to move across the first rib surface
with each breath, and its underside would be subject to friction. This
paper postulates that over the course of three hours, the subclavian
artery became abraded, injured and its wall attenuated, until finally the
artery ruptured and profuse bleeding ensued. It is likely that bleeding
was directed downwards and caused a large tension haemothorax (figure 2),
as occurred in rupture of a subclavian aneurysm reported in the
literature.[4] Tension haemothorax can contain up to 40% of the
circulating blood volume [5] and may lead to fatal circulatory
collapse[6].
In terms of the effusion of water, Hébert-Blouin et al have documented
tracking of cerebrospinal fluid (CSF) to the ipsilateral paraspinal and
peripleural space adjacent to the upper lung following brachial plexus
injury. They showed accumulation of CSF in the paraspinal and superior
peri-pleural spaces on imaging (figure 3).[6] There is normally about 150
ml of CSF which is produced at a rate of 20 ml per hour. An extensive tear
in the meninges associated with a brachial plexus avulsion is likely to
have drained most of the intracranial CSF. Over the ensuing 3+ hours from
the time of injury until death, a further 60 ml could have drained giving
the potential CSF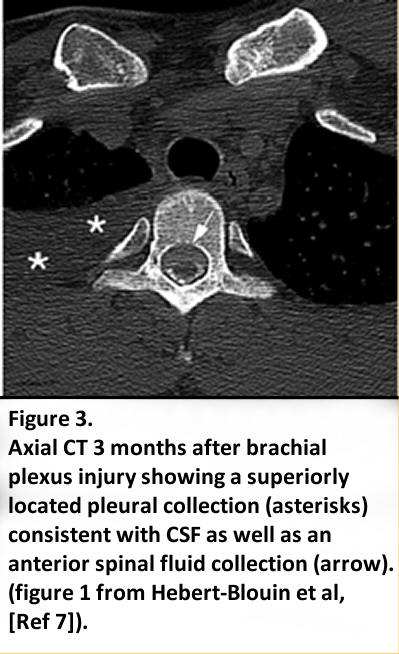 loss of over 100ml. It is postulated that the lance perforated into a
peri-pleural collection of cerebrospinal fluid (Figure 3) and effusion of
clear fluid resulted.
loss of over 100ml. It is postulated that the lance perforated into a
peri-pleural collection of cerebrospinal fluid (Figure 3) and effusion of
clear fluid resulted.
What is uncertain however is whether a peripleural CSF collection
could form within such a short period of time after an injury, as the
reported cases with peri-pleural collections were only scanned weeks or
months after the injury.vi It may be that the repeated body movements
needed for the forced exhalation during crucifixion encouraged downwards
tracking of CSF. Loss of CSF from brachial plexus avulsion is associated
with low pressure headache, a further potential source suffering for the
crucified Christ.
Figure 3. Axial CT 3 months after brachial plexus
injury showing a superiorly located pleural collection (asterisks)
consistent with CSF as well as an anterior spinal fluid collection
(arrow). (figure 1 from Hebert-Blouin et al, [7]).
The Rev Professor Patrick Pullicino is a Secular Priest of the
Southwark Diocese and a retired Professor of Neurology
References:
- Bevilacqua M, Fanti G, D’Arienzo M, De Caro D. (2013) Do we really need new medical information about the Turin Shroud? Injury. Int. J. Care Injured 45: 460–464.
- Bevilacqua M, Fanti G, D’Arienzo M. (2017) New Light on the Sufferings and the Burial of the Turin Shroud Man. Open J Trauma 1: 047-053.
- Edwards WD, Gabel WJ, Hosmer FE. (1986) On the Physical Death of Jesus Christ. JAMA The Journal of the American Medical Association 255: 1455- 63.
- Foudrain A, Lafitte S, Iquille J, De Dominicis F, Berna P. (2017) Delayed-onset tension hemothorax following blunt trauma and the rupture of a previously undiagnosed aberrant right subclavian artery. J Thorac. Dis. 9: E245–E248.
- Pumarejo Gomez L, Tran VH. Hemothorax. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK538219/
- Zeiler J, Idell S, Norwood S, Cook A. (2020) Hemothorax: A Review of the Literature. Clin. Pulm. Med. 27: 1–12.
- Hébert-Blouin M-N, Mokri B, Shin AY, Bishop AT, Spinner RJ. (2013) Cerebrospinal fluid volume–depletion headaches in patients with traumatic brachial plexus injury. J Neurosurg 118: 149–154.