
Catholic Medical Quarterly Volume 58 (2) May 2009, 19-28
The Spiritual Care of dementia
Dr Adrian Treloar FRCP, MRCPsych MRCGP
Consultant and Senior Lecturer in Old Age Psychiatry
 This article is based upon a talk originally given to Extraordinary
Ministers of Holy Communion. It started with a recording of the Catholic Hymn
“Hail Queen of Heaven”.
This article is based upon a talk originally given to Extraordinary
Ministers of Holy Communion. It started with a recording of the Catholic Hymn
“Hail Queen of Heaven”.
Spiritual care is widely recognised as being crucial in the care of those with dementia and those who are dying but the concept of spiritual care is poorly understood and poorly supported. Many are inclined to think that it is about making people feel better, providing comfort and support and enabling understanding. Whilst this is of course true, having thought this through this I became aware that that is not enough.
There must also be a religious and spiritual component for those who want and need it. As I thought about all this I came across a hymn which, for me, gives a sound and sensible philosophical and practical basis for understanding what spiritual care is. It comes from the Catholic “stable”. But it might just as well apply to any other Church or Faith stable with a bit of adaptation.
The hymn sets out how the gentle, kind and nurturing support, that all people of faith must wish to bring to those who are dying, must be set out alongside a clear understanding of the structures which that faith brings to provide such comfort and care. Put together, good spiritual care becomes a powerful tool for many.
It is true that the model may have some limitations for atheists, but for agnostics, we know that, as death and crisis nears, the acceptance of the possibility of the supernatural generally increases substantially. Even for atheists, we must allow those who are dying to hope in the future, even if they cannot believe that that future will simply not include them.
Our Lady Star of the Sea
 There is a hymn which, for me, sets out that basis of understanding. It is a
hymn to Our Lady, Star of the Sea called “Hail Queen of Heaven”. Of course it is
not a hymn about dementia. It is in fact a hymn written in the 18th century at a
time when sailors were regularly subjected to massive storms, while sailing in
small wooden ships around the world. They routinely knew what it was to fear for
their lives upon the sea and routinely knew the prayers they would say as they
hoped to survive the storm. On such nights, storm tossed sea sailors would look
to Our Lady to keep them safe, to protect them and to bring them home safely to
their families. The stars (especially the North Star) are the guide for sailors
and it is natural therefore for Our Lady, who is the guide and protector of
sailors at sea, to be seen as the “Star of the Sea”. So it is that for sailors,
who may be more regularly frightened and terrified for their lives than any
others, Our Lady becomes their guide and protector in those darkest and
stormiest nights.
There is a hymn which, for me, sets out that basis of understanding. It is a
hymn to Our Lady, Star of the Sea called “Hail Queen of Heaven”. Of course it is
not a hymn about dementia. It is in fact a hymn written in the 18th century at a
time when sailors were regularly subjected to massive storms, while sailing in
small wooden ships around the world. They routinely knew what it was to fear for
their lives upon the sea and routinely knew the prayers they would say as they
hoped to survive the storm. On such nights, storm tossed sea sailors would look
to Our Lady to keep them safe, to protect them and to bring them home safely to
their families. The stars (especially the North Star) are the guide for sailors
and it is natural therefore for Our Lady, who is the guide and protector of
sailors at sea, to be seen as the “Star of the Sea”. So it is that for sailors,
who may be more regularly frightened and terrified for their lives than any
others, Our Lady becomes their guide and protector in those darkest and
stormiest nights.
Verse 1
Hail, Queen of heav'n, the ocean star,
Guide of the wand'rer here below;
Thrown on life's surge, we claim thy care:
Save us from peril and from woe.
Mother of Christ, O Star of the sea,
Pray for the wanderer, pray for me.
So the first verse of this hymn sets out the vision of Our Lady as the
guide of the sailor thrown upon the sea. The verse pleads with her to save them
from peril and from woe, bringing them safely home to port. But inevitably when
people who work with dementia sing this hymn they are bound to smile a wry smile
when they pray for the wanderer. Dementia is, after all, a condition which
causes more wandering than any other medical illness.
Verse 3
Sojourners in this vale of tears,
To thee blest advocate, we cry;
Pity our sorrows, calm our fears,
And soothe with hope our misery.
Refuge in grief, star of the sea,
Pray for the mourner, pray for me.
Mother of Christ, O Star of the sea,
Pray for the wanderer, pray for me.
But here in Verse Three we see what Our Lady does for sailors at sea.
What is it that the terrified man would look for in the mother of Our Lord?
Actually he would look for someone who is able to understand his needs and able
to understand how to help someone who is in such fear. Someone with dementia who
is unable to remember or understand what is wrong with them will also look for
the same qualities both in Our Lady and in those who set out to provide
spiritual care for them.
We cry out to Our Lady to take pity upon our sorrows, to calm fears, to
sooth our suffering and to give us hope. We ask Our Lady very simply to pray for
us; to pray for the wanderer; to pray for the person with dementia. So it is
that we should set out to provide care for people with dementia.
Verse three is literally a manifesto for the spiritual care of people
with dementia.
The need for spiritual care of dementia
Of course it is simply a necessity that we should support and care for people
with dementia. By doing so we not only help them, but we are helped ourselves.
We are truly dignified by the care which we show to the most vulnerable members
of our society. Just as Mother Teresa was hugely dignified by the love she
showed to deserted children, we too are dignified by what we do for those who
need us most.
To do this better we must of course understand the problems faced by the people we seek to help. We must understand about dementia and learn a little as to how we provide good care. Then we will be able to give effective spiritual care as well.
Living well with dementia
It is worth noting that it is quite possible to live well with dementia. For
some, dementia is not actually a distressing illness. For some the worries of
being responsible, running a family, worrying about finances and dealing with
all the conflicts of life is reduced by becoming forgetful. Some people actually
become happier as a result of dementia than they were before they got it.
 Many more can indeed be perfectly happy with adequate care support and
love. There is a massive difference between somebody who is struggling, hungry,
with mouldy food in the fridge and an unheated house and somebody who is cared
for, is warm and clean and has food and company. The latter may well be
perfectly happy while the former will struggle greatly. The difference between
the two is procured entirely by right minded people giving good care. Dementia
requires that we provide the right care and support to those who suffer it, so
that they can live as well as possible and be comforted in their illness.
Sometimes this can be excellently achieved in their own home and often with
their own families. Other times it is best achieved in care homes. Sometimes it
needs medication in addition. Wherever somebody with dementia is looked after,
they really do require the best possible care.
Many more can indeed be perfectly happy with adequate care support and
love. There is a massive difference between somebody who is struggling, hungry,
with mouldy food in the fridge and an unheated house and somebody who is cared
for, is warm and clean and has food and company. The latter may well be
perfectly happy while the former will struggle greatly. The difference between
the two is procured entirely by right minded people giving good care. Dementia
requires that we provide the right care and support to those who suffer it, so
that they can live as well as possible and be comforted in their illness.
Sometimes this can be excellently achieved in their own home and often with
their own families. Other times it is best achieved in care homes. Sometimes it
needs medication in addition. Wherever somebody with dementia is looked after,
they really do require the best possible care.
Distress in dementia
 For many others dementia is a distressing condition and here is a picture of
a lady who was extremely distressed, struggling and frightened when we started
caring for her. It is important that we do what we can to alleviate the distress
and suffering of people like this. Just as surely as we must treat the pain of
people dying with cancer, we must also seek to effectively alleviate the
suffering of those with dementia. The good news is that we can usually do this
fairly well although the reality is that we often fail to achieve this as well
as we should: people often do not get as much care, assessment and understanding
of their needs as they should.
For many others dementia is a distressing condition and here is a picture of
a lady who was extremely distressed, struggling and frightened when we started
caring for her. It is important that we do what we can to alleviate the distress
and suffering of people like this. Just as surely as we must treat the pain of
people dying with cancer, we must also seek to effectively alleviate the
suffering of those with dementia. The good news is that we can usually do this
fairly well although the reality is that we often fail to achieve this as well
as we should: people often do not get as much care, assessment and understanding
of their needs as they should.
This lady was living at home with her husband with good care and
support, having had medication adjusted appropriately and with the right
assistance in terms of other carers and trips out
 etc. Her husband was delighted
she was at home and would send me pictures such as this as a token of his
gratitude. Indeed he was so pleased that he asked me to show pictures of her at
talks like these.
etc. Her husband was delighted
she was at home and would send me pictures such as this as a token of his
gratitude. Indeed he was so pleased that he asked me to show pictures of her at
talks like these.
It turns out that in fact the two ladies in the two slides are the same person. The surprise is that the top picture is her in 1995 and the bottom picture is her in 1997. She got better as a result of good care and a large part of her recovery was due to her return to her own home from the nursing home and the prescribing of appropriate medication etc.
For her the best care made her better but it is worth pointing out that
often enough the best care will be to palliate (alleviate?) the distress, accept
much of the decline which is associated with dementia and seek to provide the
best comfort and care right through until death. Dementia is indeed a condition
which causes death and on average people have about four and a half years after
it is diagnosed. There is a wide variety of life expectancy (some live much
longer) but the notion that dementia does not cause death is a false one.
Dementia leads to inactivity, reduced resistance to illness, and an increased
risk of strokes, heart attacks, pneumonia etc. Painful and difficult treatments
become rightly limited and as a result death comes sooner to those who have
dementia.
So it is right to be sure that we reduce distress in people with
dementia when they are distressed but at the same time cherish and encourage
them in every way we can.
The opportunity for us to care
But for everybody with dementia the illness provides an opportunity for others to support the sick and to help them to prepare both spiritually and socially for the end of their lives. Indeed this is an opportunity which is often not available to those who die suddenly and unexpectedly.
Dementia also requires anybody who gets it to accept care and support in ways in which they may previously have never done. Personal care, washing, cooking, being fed, accepting some of the indignities of being changed and having accidents are part of the illness (although that perception as an indignity is value based: accepting care can demonstrate the worth of the person cared for who is thus dignified).
In a Christian sense we must accept that all those whom we feed, all those whom we clothe, all those whom we visit when they are sick and all those whom we visit in care homes take the place of Christ as we care for them (Matthew 25, 36). Each person with dementia gives us the opportunity to love Christ by serving the people he loves so much. We are also supporting those whom he expects and hopes to take to him so soon.
What is dementia
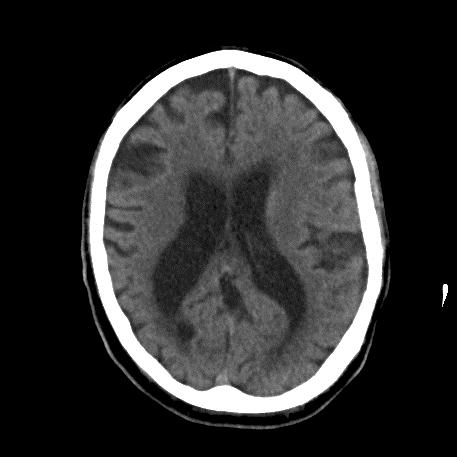 Dementia is a progressive condition associated with the loss of brain cells.
The underlying pathological process causes brain cells to die and the
connections between brain cells to become reduced. As a result the entire brain
functions less well. As well as difficulties in memory there are changes in
personality, reduced ability to do things, reduced understanding and a reduced
ability to communicate.
Dementia is a progressive condition associated with the loss of brain cells.
The underlying pathological process causes brain cells to die and the
connections between brain cells to become reduced. As a result the entire brain
functions less well. As well as difficulties in memory there are changes in
personality, reduced ability to do things, reduced understanding and a reduced
ability to communicate.
The picture shows a brain scan of someone with a combination of Alzheimer’s type dementia and a vascular dementia. The amount of brain (which is grey) is reduced. The black shadows in the middle are the ventricles which are enlarged and the black lines around the outside show the increased gap between the folds of the brain. This person has a moderate dementia. In severe dementia changes are often more marked.
In Alzheimer’s disease you see microscopic things called Neuro-fibrillary
tangles and plaques. It is these microscopic processes which cause the brain
cells to become disordered and to die.
In vascular dementia small blood vessel disease causes tiny infarctions (small areas of cell death) and hundreds of thousands of these areas combine together to produce a similar effect. If there is a difference between the two dementias, it is perhaps that insight is often a little more present in vascular dementia and then maybe sometimes more focal deficits in ability.
Most dementias are a mixture of those two types.
There are various types of dementia. We have already mentioned the
Alzheimer’s type and the vascular type. There are dementias associated with
Parkinson’s disease, and also rarer forms of dementia such as Picks disease or
fronto-temporal dementia.
It is worth just mentioning that it is the Alzheimer’s type and the
Parkinson related dementias that appear to benefit most from the memory
improving medications.
Need for care in dementia
The greatest need in dementia is really good care. Without care people will
suffer in pain or distress and discomfort. Support is so much more effective
than any other medication or treatment. Sensitive support, understanding,
communicating well and respecting and loving is absolutely essential.
Good treatment does include memory improving drugs but will also include excellent medicine optimising all the other conditions the patient has. In addition, alongside the highest standards of care and support, distress must be alleviated. Sometimes this requires medication. Other times it just requires good quality care.
The need for hope, trust and faith
Of course all those with a life limiting illness should be able to have hope
and trust that their care will be excellent and those looking after them will do
the very best they can.
In all honesty, patients with dementia have the right to expect ongoing
care and support from both professionals and clerics, as well as from those who
value their faith and appreciate what their faith means in terms of the call to
charity.
People with dementia must always be respected and should not be seen as an encumbrance. I have seen people with dementia in the last days of life continuing to contribute to those around them and continuing to function as a member of a family. We too easily conclude that those who are dying no longer serve those who will be left behind. Even at the very end of life, we can see a two way relationship between the patient and carers.
Communication
It is worth mentioning that communication is a really important issue in dementia care. Anyone visiting the sick needs to take time and they need to be relaxed. Try not to be too complicated. It is a real blessing to be able to enjoy the person you are with. If you know more about their background this becomes easier. It makes it possible to do things differently and people with dementia remember the past much better than they remember the present. In this context discussion about the past may well be helpful.
A gentle chat about Church last Sunday will remind the individual of their trips to Church throughout their life. Gentle chats about anything relatively trivial will give a calm and relaxing atmosphere enabling the best communication and the best quality of interaction.
People with dementia become distressed when they cannot understand. They equally become distressed when they cannot work out how to reply to somebody. So it’s really important to try and avoid arguments. It’s also useful to try and put the answers into questions. Rather than saying “do you want Holy Communion”, it is perhaps a little better to try something like “it’s my day for visiting you and so I brought you Holy Communion.” The latter may well get a far more positive response.
It is not enough to be just caring and nice
It is very definitely not enough just to be nice caring and comforting. Dementia brings the need for real changes as life is truly changed. Dementia also brings the opportunity to think and pray about these changes. Given that someone with dementia is no longer as able to practice their faith by themselves, it is really important that we provide them with the opportunity to do so.
By doing so we will help to value and respect them as we should. If we
leave them alone, we neglect our Christian duty.
Spiritual care of dementia
Indeed most of all dementia is a social and spiritual illness. While we focus mainly upon the medical, it is about a profound change in life and also unquestionably about the final journey of individual sufferers towards God. So if we neglect the spiritual, we fail our patients.
In fact health services almost always forget the spiritual and will almost always only send for the Church at the last moment if they ever do at all. Priests and Church visitors are excluded from the confidential network of hospitals. Therefore they are never told there are Catholics in hospital: they must tell us themselves. People with dementia cannot do this and nor can other very sick individuals. It is really important therefore that we keep an eye open for all those whom we know so that we are informed when they go into hospital and when they go into care so that we can provide the right input and right support for them. What a tragedy it is when the sick and vulnerable members of our society are thus denied access to the spiritual care they should have a right to receive.
I remember when I first qualified taking a couple of people to Mass on
Sunday at a time when there was a Mass in the hospital. A few days before a lady
had collapsed unconscious with a cardiac arrest. Happily she survived, though
she was very ill. Seeing me taking others to Mass she asked if I could take her
too. I told her “no” because she was too ill. She was still there the following
Sunday and she called me over to ask if I would take her this week. After Mass
she burst into tears and told us that she had not been to Mass in 40 years. It
was a beautiful afternoon!
Sacramental and prayer support of dementia
We should not forget that there is plenty of evidence that prayer works. Even the doubters at the very least cannot say that prayer does not work. So we need not apologise for praying with the sick and we need to be able to help some people to pray and to guide them towards prayers that fit the needs that they have.
Of course if prayer works (which we believe that it does), it does more
than to just comfort or make us feel good. It can make a real difference and
lead to real changes for individuals.
Sacraments
Beyond that of course the sacraments are real means of actual concrete grace and these must not be neglected or denied to the sick. In baptism we are born to Christ, and in Holy Communion Catholics believe that they truly receive the body of Christ. In Confession their sins are forgiven (by Christ) and in the Anointing of the Sick they are given the strength, peace and courage to overcome the difficulties that go with the serious illness or frailty of old age as well as prepared in a special and spiritual way to meet Our Lord. Sins are also forgiven by the sacrament of the
Anointing of the Sick
Through all the sacraments we are helped further along our path of redemption by Christ our Saviour.
Confession
 Confession does require an awareness of sin, an understanding of repentance,
and the ability to articulate both the sins and the repentance. Confession is
quite possible to do early on in dementia but in advanced dementia it will
really become quite impossible.
Confession does require an awareness of sin, an understanding of repentance,
and the ability to articulate both the sins and the repentance. Confession is
quite possible to do early on in dementia but in advanced dementia it will
really become quite impossible.
So, let’s think about things early rather than leave it too late. Let’s consider offering confession to those with early dementia who are Catholic rather than forgetting the spiritual needs of our patients until it is too late.
A note here - it is worth mentioning that people do some remarkably
inappropriate things when they have dementia. Perfectly decent kind and saintly
people will start hitting, spitting, swearing and stripping off. I have had
wonderfully good Catholics telling me to do things in very colourful language.
 These are almost certainly not sins. They are not wilful acts but they reflect
acts of disordered minds and we may console ourselves and their families with
the thought that they are done in the innocence of dementia. Indeed in the
circumstances people with dementia are probably just as innocent as a
one-year-old.
These are almost certainly not sins. They are not wilful acts but they reflect
acts of disordered minds and we may console ourselves and their families with
the thought that they are done in the innocence of dementia. Indeed in the
circumstances people with dementia are probably just as innocent as a
one-year-old.
So offer Confession early while people can understand the issues of dementia.
The ability to receive Holy Communion
To receive Holy Communion requires the proper dispositions for receiving Holy Communion. It also requires an understanding and belief that this is something special. It is not necessary to have the full understanding that the host is truly the Body of Christ although this is, of course, desirable and hoped for in communicants who do not have dementia. In the case of someone with learning disabilities it would only be necessary to establish that they knew the difference between the Eucharist and ordinary bread - "a belief that is it something special". As a result it may not be suitable for those with very severe dementia and it can be problemmatic for people who spit it out. Generally one is likely to assume that if people spit out the host they are failing to understand what is offered. If there is doubt, then perhaps a very small fragment of a host is a good idea. Our Blessed Lord’s body is equally present regardless of the size of host given.
If you were to ask a person who is a devout Catholic whether they would wish to continue receiving Holy Communion if they reached a point where they unwittingly spat out the sacred host, they would surely say that they would not wish to receive the Sacred Host in those circumstances. This is not a question of a person being "unworthy" but of respecting the dignity of someone who has always lived a devout Catholic life.
On the other hand I once took a lady to Mass with a quite severe dementia which caused her quite a lot of distress. She chatted all the way through Mass and looked somewhat distressed. However, at Communion she stilled and became calm. It was not only me who thought that a significant spiritual change came upon her at the time she received Communion.
So the bar to receiving Communion is really quite low but if you clearly expect that giving it will cause the Host to be spat out etc., then perhaps it is best to pray and not actually give Communion.
Finally if the Host is spat out then you can probably consume it yourself. You may not like doing this but it is pretty safe and the infections you might get very rare. There is no evidence that you could contract dementia by doing this and it will protect the Host from further indignity. The alternative is (remembering it to be truly the Body of Christ and thus due very special reverence) to take it back to Church and to put it is a glass of water beside the Tabernacle until it no longer has the form of bread. By then it can be disposed and the recommended method for this is to dispose of it into the sacrarium or directly into the ground if the Church does not have one, and not down a drain etc. While to some such caution may seem daft, it does in fact enable us to show the extreme love and reverence we wish to have for Christ our Saviour.

Anointing of the Sick (formerly referred to as "Extreme Unction")
The sacrament of Anointing of the sick is for people with serious illness and
life-threatening illness, including old age. It can be received more than once
during the same illness if the patient’s condition becomes more serious, or in
the elderly whose frailty becomes more pronounced. It is best not left to the
last minute. Clinicians and Extraordinary Ministers should seek to ensure that
those who are unable to ask for Anointing themselves are provided with the
opportunity to receive it. [1]
Prayer
 Prayer is so important. We remember from Verse Three of the hymn we discussed
at the beginning, the importance of comforting and soothing the worries and
fears of our patients. Prayer is a practical thing that we can do and even in
very advanced dementia we find patients responding to it, joining in and doing
other acts of devotion as a result of the prayer they are surrounded by. I
remember a lady the night she died: the family said prayers at her bedside and
during the last decade she made a tiny but perceptible sign of the cross. Many
others have shown similar signs of response. It was the last sign of awareness
that she ever gave.
Prayer is so important. We remember from Verse Three of the hymn we discussed
at the beginning, the importance of comforting and soothing the worries and
fears of our patients. Prayer is a practical thing that we can do and even in
very advanced dementia we find patients responding to it, joining in and doing
other acts of devotion as a result of the prayer they are surrounded by. I
remember a lady the night she died: the family said prayers at her bedside and
during the last decade she made a tiny but perceptible sign of the cross. Many
others have shown similar signs of response. It was the last sign of awareness
that she ever gave.
Remember that even when people are unable to respond they may well hear and understand what is happening. This has certainly been the message given by people who have been apparently unconscious and recovered (from conditions other than dementia which you cannot recover from)
Remember too the widely held hypothesis that perhaps prayer may be more effective when it is offered by someone who is really suffering.
There are many forms of prayer but some of the simplest and most familiar will be good. The Our Father, the Hail Mary, the Creed. The Rosary takes a little longer. Actually that may be quite a good idea because 20 seconds of prayer may not be enough to produce the calm understanding and the oneness with God which the Rosary can offer. So if someone cannot receive Communion etc., then a few decades of the Rosary said at their bedside may well be really helpful.
For others, reading from Scriptures or text from the writings of the saints may
be really helpful.
Prayers for the dying
There are some beautiful prayers in the St Andrew Bible Missal for those who are dying and these are available on the Internet and easily downloaded. They help both the dying and bereaved. The litany of prayers has been said by many people who we know and can be very helpful.
The prayers for those who have just died give the opportunity to see how the soul is carried forth from the body to meet Our Lord and the final judgement. Of course it is right to pray for these people on their last journey and to pray for their forgiveness by their Saviour.
You can find some prayers which many have found to be really helpful at
www.cmq.org.uk/Miscellaneous/Prayers_for_the_dying.pdf [2]
Or just put “catholic prayers for those who are dying” using quotation marks
into Google and you will find it.
Late illness awareness
People who are dying may often seem to be unconscious or semi responsive. We know that often enough there is good awareness and that even though there may be no response, they will participate in prayers and listen. The prayers below may be said therefore, firstly because they are effective prayers to help the dying on their journey to meet Our Lord and secondly because, if said aloud in the presence of the person dying, that person will know those who care and love them are near. They may of course be said more than once, though the time they allow you to spend praying with the person who is dying will mean that frequent repetition is not required. [extracted from Catholic Prayers for those who are dying or who have just died]
We mentioned earlier the late illness awareness of some of the patients we have known.
Assume the patient can always hear you and be aware until they are actually dead, by which time they may see you praying for them as their spirit leaves their body. Pray with them and for them.
Sometimes use words and set prayers. But sometimes use quietness too, though words give a structure to communicate the peace of Christ.
Mistakes we make
I think I should also mention some of the mistakes we make in terms of looking after people with dementia and other mental illnesses. Christianity is a wonderful thing which brings wonderful support but we do have to understand when we get things wrong.
Firstly of course there is the question of the sins of our Fathers and the sins of our past. Our Lord specifically discounted the hypothesis that our illnesses are caused by the sins of our Fathers. Similarly most illnesses simply arise as a result of illness and not the things we do wrong. Mental illness is really not very different from other illnesses.
Sadly many people subscribe to the idea that depression is in fact a sign of emotional or spiritual weakness. This can lay a very heavy extra burden upon those who suffer such illnesses.
 So I do find myself feeling very distressed when I see a poster like the
one in the picture stuck up outside a local church and saying “If you have no
hope then you have not found Jesus”. To suggest that those who have a depressive
illness have not found Jesus is to tell them they are to blame for their
depression. This is really deeply insensitive and quite unchristian. It is
factually wrong and misses entirely the duty we have to care for those who are
ill. Depression is a major illness which does indeed remove the hope of those
who suffer it. I have met many good and wonderful people of strong faith who,
through having got a depressive illness, have indeed lost their hope in the
future and even lost hope of salvation. Theirs is a grave cross and we should
not add to it by telling them they are imperfect or bad Christians.
So I do find myself feeling very distressed when I see a poster like the
one in the picture stuck up outside a local church and saying “If you have no
hope then you have not found Jesus”. To suggest that those who have a depressive
illness have not found Jesus is to tell them they are to blame for their
depression. This is really deeply insensitive and quite unchristian. It is
factually wrong and misses entirely the duty we have to care for those who are
ill. Depression is a major illness which does indeed remove the hope of those
who suffer it. I have met many good and wonderful people of strong faith who,
through having got a depressive illness, have indeed lost their hope in the
future and even lost hope of salvation. Theirs is a grave cross and we should
not add to it by telling them they are imperfect or bad Christians.
Depression is in fact a medical illness. It is not a sign of a lack of faith but is actually in most people, a predisposition to illness caused by either inbuilt or inborn traits or acquired illnesses. The majority of depressions in old age arise from small blood vessel disease in the brain. So we need not concern ourselves with working out why people are depressed etc. Schizophrenia too is an illness which has an essentially inborn cause. It is not an illness which you get because you have bad parents or because you do bad things yourself. If we get pneumonia we consider ourselves unfortunate. It is far easier to give ourselves pneumonia than it is to give ourselves schizophrenia or depression.
In depression people may start to believe and worry about awful things. In the elderly their past will come back to haunt them. It’s best to remember this. The preoccupations, beliefs and worries of a depressed person are not the cause of the illness. The illness causes them to become preoccupied about some of the bigger worries they had from earlier life. We must not attribute illnesses in old age to things from early life.
In my experience people of faith show two versions of severe depression. In one form they merely conclude that their sins have been so awful that they cannot possibly be redeemed and they become convinced of their damnation. Even a minute tax error in the early 1950’s can provide enough evidence to support an unshakable belief in their damnation. The other group merely lose their faith and conclude that all they ever did was in vain. Either form of depression is a huge torment. Tell them it is their fault for lacking faith and you merely enhance their suffering.
Dementia is not a punishment from an earlier life, it is merely an illness acquired in old age.
Remember too that pain due to a broken leg would never be treated by love, a hug and a cup of tea. We will splint it and mend it. The pain of that leg may be reduced a little by love and good care but it will not be effectively treated.
In the same way the distress of dementia also requires good effective treatment along with the right love and support. To try and treat the distress of dementia without the right medication should be just as unacceptable as trying to treat a broken leg with prayer but no splint.
Final tips
- Be confident but humble.
- Be confident that by caring you do what is good and what God wants.
- Be humble knowing that in doing your best, you will both succeed and get it wrong.
- Try and find out a bit about the person you’re caring for: it will help you care better.
- Do not fight.
- Offer care and love.
- Cherish the dying and love the sick.
- In the midst of the work and strain of it, try to enjoy the privilege of providing care for the person who is in your care.
Sojourners in this vale of tears,
To thee blest advocate, we cry;
Pity our sorrows, calm our fears,
And soothe with hope our misery.
Refuge in grief, star of the sea,
Pray for the mourner, pray for me.
Mother of Christ, O Star of the sea,
Pray for the wanderer, pray for me.
References and further reading
- Do I have a duty to arrange for my Catholic patients to receive Communion/Sacraments for the dying? Catholic Medical Quarterly Aug 2011
- http://www.cmq.org.uk/Miscellaneous/Prayers_for_the_dying.pdf
- Dementia. From advanced disease to bereavement. Oxford Specialist Handbook edited by Pace V, Treloar A and Scott S. Oxford University Press, 2011
- Adrian Treloar, Monica Crugel and Dimitrios Adamis. Palliative and end of life care of dementia at home is feasible and rewarding. Results from the `Hope for Home' study. Dementia August 2009 vol. 8 no. 3 335-347. http://dem.sagepub.com/content/8/3/335.abstract and http://www.hopeforhome.org.uk/dementia-parkinsons/research-study
- http://www.hopeforhome.org.uk
- Assessing and Managing Distress and Pain in Severe Dementia http://www.dovehouse.org.uk/document.doc?id=805